The Gesret method : the segmental man
The segmental man
Among all vertebrates, we meet, at a particular stage of the embryo development, mesodermic formations following each other that we name metameres or primordial segments.They are considered as a phylogenetic representation of the invertebrata body structure, particularly the annulated.
The segmentation of the embryo goes back to the first phases of its development. Around the 15th day (about 2 mm) the first metameres appear (cervical vertebras to be) and around the 25th day (about 5 mm) they will count 35.
From this very stage cells will separate from the neural crest to constitute two parallel cords.
One will give birth to the previsceral plexus or ganglions, the other to the laterocervical chain of the spinal ganglions. Around the end of the 3rd month the segmentation of the ganglionic masses will be over, strictly responding to the rachidian pairs from which they come. This "rosary-like" shape will turn, in some places, into a "pod" integrating a few "beans" to constitute the masses of the stellar, thoracic and lumbar ganglions.
The sympathetic system is the basic element of the nervous system
- It is the oldest in the ontogenic order as well as the phylogenetic order; its starting mode is previous to the cerebrospinal system one: the visceral plexus precedes the brain. (Guy Lazorthes)
The spinal ganglion
The sympathetic system, more specifically the laterovertebral ganglion, plays a prominent role:
- It makes the peripheral projection of an autonomous impulse possible but it remains under the influence of the anterior hypothalamic function.
It offers something of major interest. Thanks to it we are now able to define briefly the following three neurological entities:
- the myotome, governed by the somatic motor neuron
- the viscerotome, governed by the autonomous motor neuron
- the dermatome, governed by the juxtaposition of the exteroceptive protoneurone and the peripherical deutoneurone.
The three of them depend upon the same medullary segment or myelomere.
of cutaneous reflexotherapy in its various forms, on the basis of our western
knowledge of embryo-anatomo-immuno-neurophysiology.
Metamerized segmentation
It is obvious that interactions do exist between skin, viscera and muscles inside one and same metamerized segment.
Some people will raise the objection that metamerized segmentation is extremely vague because segments overlap just like tiles on a roof; it is therefore difficult to attribute such or such sector to a particular metamere.
About this matter Guy Lazorthes has said:
- The radicular topography of deficiency (Scherrington, Forster) has permitted to bring to light the area innervated by the direct root section. The upper and lower roots section has also brought the maximum area to light but the radicular topography is more valid.
As far as metamerized areas are concerned we can observe the differences between the following diagrams.
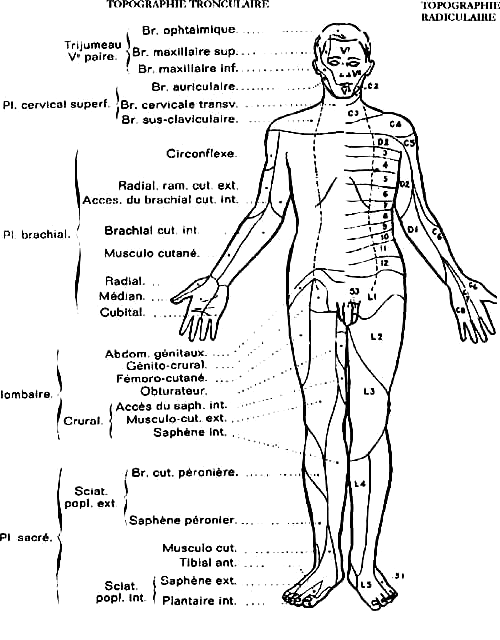
Guy Lazorthes |
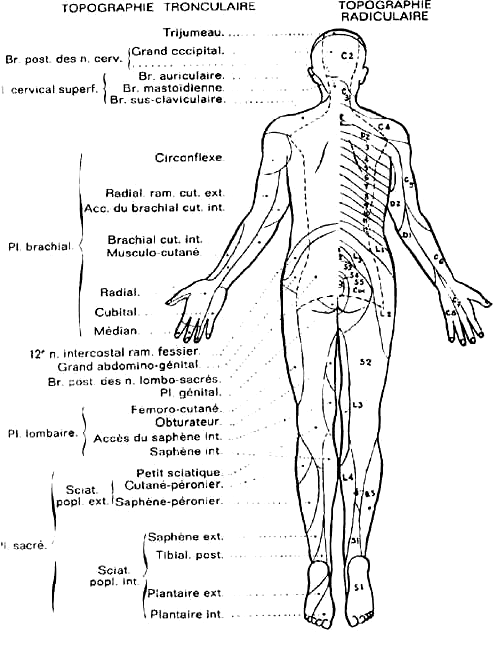
Guy Lazorthes |
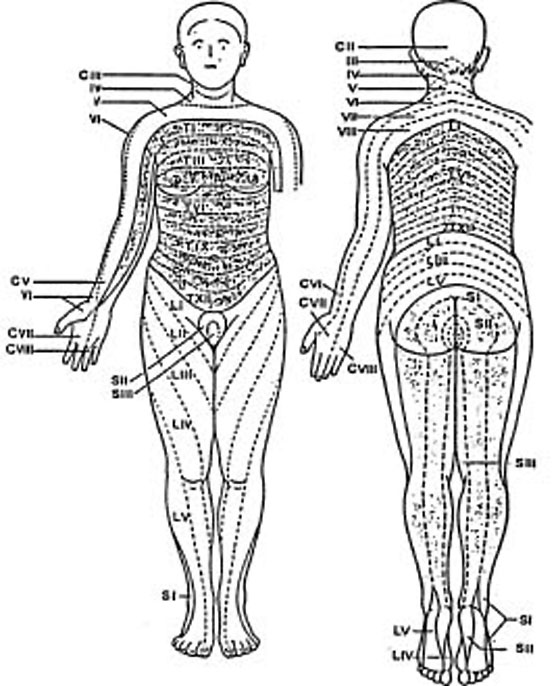
W. Kahle |
As for myself, I refer to the diagram worked out by W. Kahle from the hypaesthesic deficiencies caused by a slipped disk. (Anatomie du système nerveux, éditions Flammarion, Paris)
Aberrations of the epicritic cutaneous reflex
Using the "plum tree flower" (a traditional Chinese tool looking like a small flexible hammer whose head bears seven fine needles) I noticed that this acupuncture instrument brought about a vasodilatation reaction in the skin areas where the patient feels "stinging" type sensations (normal areas) and a lack of erythematous reaction (sometimes even a vasoconstriction) in the areas where "burning" type sensations are received (abnormal areas).
I have therefore called those observations "aberrations of the epicritic cutaneous reflex".
The use of this tool confirms the arrangement of the metamerized segments S1, S2 and S3, materializing them under the shape of white bands (in cases of lower limbs paralysis), according to the diagram used by W. Kahle.
Spinal ganglions
The overlapping of a metamerized area with the following one and the preceding one is logical; in fact, if the being constituted with rings wants to move he must control and synchronize the movements of contraction and extension of one of his segments in relation to its nearest neighbours.
The spinal ganglions could therefore appear as "metamerized mini-brains" linked to one another for synchronization without burdening the central system with a multitude of details: they are able to cope by themselves.
They are truly mini-brains because they contain "intermediate" neurones which manage and modulate the informations between medullary neurones and cutaneous, muscular and visceral ends.
Decisions are therefore made at this medullo-ganglionic level which may induce errors: projected informations, conscious or unconscious (infact pain, cutaneous projection of a visceral information, cutaneous, visceral or muscular projection of an articular information). Those interpretation errors will lead to reactions of the central system and defensive mechanisms causing pathologies rooted in this logic.
Let us listen to Guy Lazorthes :
- The attack of an internal organ may be manifested as an added pain which is projected on the parietal cutaneous area, called dermatome, corresponding to the medullary segment or myelomere to which the sensitive passages of the organ lead.
"Projected" pain
The most famous illustration is Mac Burney's point, which is the projection of an inflamed appendix. This painful point is situated at the upper two-thirds of a line joining the anterosuperior spine of the right iliac spine to the umbilicus; it corresponds to an anterior perforating bough of the 12th intercostal nerve.
This is a widespread definition, but questions remain related this point. During my researches I made clear that this point was not the only one accounting for a projected visceral pathology; there are numerous others.
The point itself is unreliable because it is still present after the appendix has been removed; a painful point, identical in its localization principle, may also manifest itself opposite Mac Burney's, and sometimes co-existing with it!
What do they mean here?
Experience demonstrates that they correspond to a suffering in the articular level D12/L1. The proof can be found in the fact that the lifting of a restriction in the articular mobility makes it disappear at once.
Other questions then arise:
- is Mac Burney's a cutaneous projection pointing out an inflamed appendix or the projection of an articular nociceptive information?
- could this nociceptive information be registered by the central system as coming from the appendix?
- could this projected information launch a defensive inflammatory reaction at the appendix level?
This hypothesis may explain the reason why the appendix sometimes shows a normal condition during surgical operation whereas all the clinical signs on which the diagnosis is based were present: nausea, Mac Burney and Bombery test (as a surgeon friend of mine told me).
We could answer those questions by checking the presence of a restriction in the articular mobility D12/L1 in a patient showing all signs of appendix inflammation, then lifting this restriction and observing the changes in the inflammation and the symptoms.
Other reflex points
This reasoning enabled me to discover other reflex points accounting for various visceral pathologies, closely linked to articular nociceptive information.
Present before the arising of the symptoms associated with the pathology, they enable every practioner to build or confirm a diagnosis.
The painful reflex points are present in:
- the 1st thoracic metamere (MT for all pathologies associated with the immunity system)
- the 2nd MT for pulmonary problems, with hypersecretion of the nose or the eyes
- the 3rd MT: pulmonary problems with hypersecretion
- the 4th MT: cardiac or pulmonary problems
- the 5th and 6th MT: stomach problems, especially anxiety
- the 8th and 9th metameres: liver pathologies, gall bladder (on the right side), and pancreas (on the left side)
- junction of 12th MT and 1st metamere: ovarians problems.
We must note that the combination of some specific points is systematically present in some specific forms of pathologies. For example, nose and eyes allergies in the combination 1 MT and 2 MT and some asthmas. The asthmatic forms of bronchitis in the combination 1 MT and 3 MT. Eczema forms in the main combination 1 MT and 8 MT right (liver) whereas psoriasis forms correspond to the combination 1 MT and 8 MT left (pancreas).
The metamerized localization of cutaneous pathologies is always associated with vertebral levels which are the root of nociceptive articular informations projected upon those areas.
Related this matter I do assert:
The root origin of a pathological reaction in a particular area,
cannot have but one cause: the specific method of linking between
this area and the central system.
Note:
Diabetics always show an 8 MT left point which is extremely
painful and often there are varicosities in this precise area.
Another note:
Those various painful points disappear within a few days or weeks
following the lifting of restrictions in articular mobility of the
corresponding levels, as well as the symptoms of the associated
pathology, providing the latter is not degenerative and/or
non-reversible.
Visceral problems = behaviour problems
I also discovered points that suggest a systematic connection between a visceral problem and a behaviour problem. Those observations lead me to build the theory of neuro-immuno-psychology, running contrary to the present-day trend of psycho-neuro-immunology (or dermatology). Once more I assert: the root origin of a pathological reaction, in a definite area, cannot have but one cause: the specific way this area is linked to the central system.
Cutaneous damages (for exemple in eczema) cannot exist in metamerized area without a cause appearing between this area and the central system. A psychological trouble may appear afterwards but it can never be considered as the origin of the pathology.
Wilhem Reich might have been a visionary when he wrote:
- We impede the free circulation of our energy through our whole
body by creating muscular "shells", rigid or dead areas
encircling us just like rings, at various levels of the body. In
order to protect ourselves from distress as well as pleasure,
from all feelings, we block the circulation of the energy.
(L'analyse caractérielle, éditions Payot, 1971)
If I get enough time (15 or 16 hours of work a day)
I will add pages on this site to give many more explanations about
the origin of behaviour problems.
I have been working on the subject for six years in close cooperation with psychiatrists, with conclusive results.
I have attempted to get in touch with the organizations that develop the theory of psycho-neuro-immunology to communicate my researches. As I am not a member of their scientific community (once more!) they did not bother responding to my proposals.
The future will confirm the accuracy of my findings: the scientific community will discover the exact mechanism, but will not be able to publish on this subject without losing dignity, because my publications, books and copyrights, came first.
I have never asked money from anybody for presenting the results of my research. I simply want to present them to the medical scientific community (in my own country, preferably) but nobody appears to want them.