Gesret method : asthma, allergies, eczema, psoriasis, the physiology of the disease
Introduction
We will ask practitioners to study this original approach of immunising pathologies (asthma, allergies, eczema, psoriasis, etc). To begin, we will point out some elementary rules:
- The structure controls the function
The structure of the eye controls the function of sight, that of the ear: hearing, and of course the thoracic structure controls that of breathing. - The cause is at the origin of the effect
The keys to understanding the effects are to be found in the causes. (Ghazâlî. The gate vault of the lights) - The function governs the behavioural rule
disorder of a function modifies the psycho-emotional and relational behaviour of the individual.
Of these three basic rules we can deduce the following :
Let us take asthma as first example to illustrate this reasoning
Asthma was always described, and continues to be considered today, as a
response to an environmental exogenic aggression, either in the form of
an allergic hypersensiblility, or in the form of psychophysiological
problems.
To my knowledge, it was never considered as a logical response to a
stress of endogenous origin, made up of articular informations (unconscious)
of type "projected" or "phantom," resulting from chondro-costales
subluxations of the first three thoracic segments.
Sympathetic - parasympathetic nerve
In 1926, E Sergent (France), considered the possibility of implementation
of these two systems and he said:
The preponderance of the pneumogastric in the attack of asthma can be due
to the momentary inhibition of the sympathetic nerve.
Consequently, all the system of innervation of the breathing apparatus
and especially of the lung is disturbed, there is a real imbalance of the
parasympathetic nerve.
Chondro-costal articulations
Strangely enough, at the same time, there existed in Germany an
operational processing (Freund) which consisted in successfully resecting
the costal cartilages of asthmatics, with success.
These two ways were soon forgotten with the improvements made in the
development of the medicaments.
Observation of static attitude
The clinical examination of asthmatics cannot cloak in silence the
traditional phases constituted by inspection and palpation.
We always remain attached to this old principle which enabled us to
release a constant clinically: the asthmatics are carrying an
asymmetrical thoracic ampliation bearing on the first three dorsal
stages.
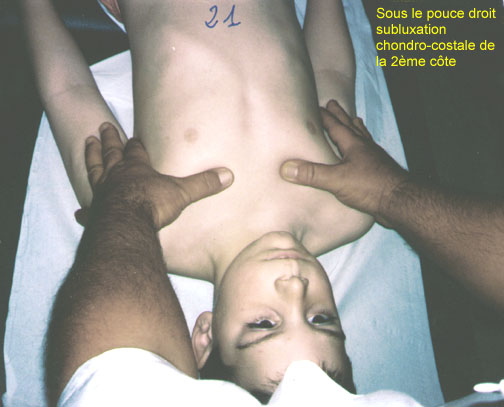
To manage this result more easily we will just simultaneously affix our
hands on both hémithorax, on the level of the synarthroses
costo-chondrales, and tell the patient to carry out deep respiratory
movements.
The comparative deficit of amplitude of one of both hémithorax observed
on its former face leads us to inspect and palpate the posterior face of
the thorax.
A confirmation awaits us there: the reduction of mobility of the first
three dorsal vertebrae.
Conclusion
It all happens as if, following a time and segmentary rotation of the top
of the bust around the rachidian axis and in a transverse plan: one of
both hémithorax was in a position of fixed posteriority.

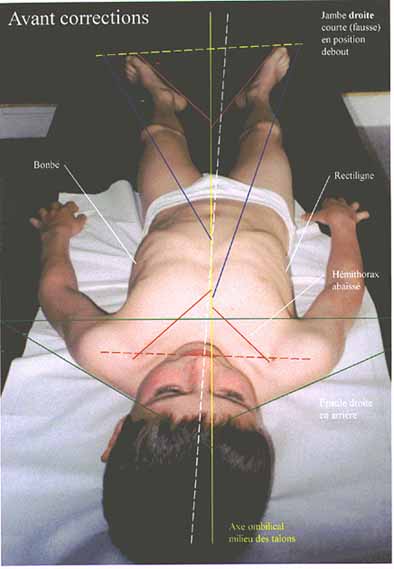
A low thorax on the
right, very visible.
A classic of the asthmatic.
(click on the picture to zoom in)
(Photo below taken before any correction.) One sees perfectly the lowering of the right hémithorax and the anomalies of the various body axes. As opposed to what one would think, it is the right leg which is short (false) while standing. The torsion of the pelvis is also seen. (These observations are constant.)