Asthma Gesret method : it is necessary to review all present principles
Introduction
The following describes an original piece of research, completely
ingnored by traditional medecine to date, and dealing with the mechanisms
of asthma and allergies: Structure paths.
The function and the structure
It takes a long time for a new function and a new structure to establish
themselves, in fact several generations. The mechanism by which this
happens is called a mutation. During the animal reign (to which mankind
belongs), and its evolution, some species expressed the desire to come
out of the aquatic life. New functions were therefore required: breathing
in air, displacement, etc. To enable those functions, news structures
were created: lungs, limbs, etc.
But, at the time, lungs were only simple, soft and fragile pockets, so a
bony superstructure, rigid and mobile, with a protection, dilation and
contaction role, set itself up.
The respiratory function in air was achieved and:
- one cannot disassociate this function from its structure!
If the respiratory structure is to be disrupted, so will the function! It is obvious. Why do we have to limit ourselves to functional exploration in the case of respiratory pathologies, Whereas in the other specialties one always proceeds to a structural exploration: ear, eye, hand, foot, etc.?
General definition of asthma
Asthma, according to literature :
- Is a respiratory hindrance provoked by a great difficulty to expire (breathe), which occurs by excess. It may appear, disappear, or persist at all ages with an unforeseeable variability. It is also conditioned by an intermittent bronchial shrinkage due to spasm of smooth muscles and an obstruction of bronchial secretions.
The main character of asthma is :
- an expiratory difficulty(dyspnea), generally evolving by strong crises (paroxystics), separated by long periods of absolute calmness.
Breathing, expiratory difficulty :
- the inspiration is short and silent, while the expiration, prolonged, laborious and loud, requires great effort.
But another sort of dyspnea exists
- The unnoticeable inspiratory difficulty, wrongly recognised as being an
asthma attack.
In this case the ruling phenomena are completely opposed
The inspiration is prolonged and loud, requiring an effort, provoking a depression of the sus-sternal bone; on the other hand the expiration is short and silent. In this case one notes that it may be characterised as a pharyngeal spasm and not of a bronchial one.
Asthma in France
There are 2.5 to 3 million asthmatics of which 1/4 are children and teenagers. Every day, just in France, 7 people die of an asthma attack: one every 3 and a half hours. This figure is higher than that related to AIDS but far less publicized.
Personal Research and Discoveries Chronology
On July 15th 1974, when he was ten years old, my son, Franck died
following an ultimate asthma attack. From then on, I haven't stopped
trying to understand why!
Faced with no answers in medical literature to my questions, I moved
towards alternative topics: auriculotherapy and Chinese traditional
acupuncture.
From 1980, I started practicing these disciplines, until 1984, the date
at which I moved house and settled in Bayonne. It is there that I made
observations which pointed at the understanding of pathologies such as
allergy, asthma, eczema and psoriasis.
I discovered that all these pathologies shared a common factor with slight variations, making them unique: a malfunctionning of the structure, starting with unaligned hips resulting in a compensatory habit placing the upper part of the thorax in a position of fixed rotation.
In more than 90% of cases, people suffering from asthma have the right side of the thorax well lower than the left. This is clearly apparent when placing the patient on his back.
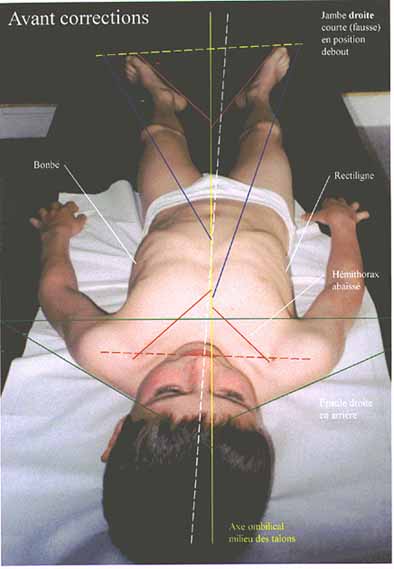 One perfectly distinguishes in the photograph (the child being in an
upright position) other anomalies frequently observed in people with
asthma:
One perfectly distinguishes in the photograph (the child being in an
upright position) other anomalies frequently observed in people with
asthma:
lowering of the right part of thorax (in more than 90% of cases); tilted
head (opposite direction to the leg referred to as "short"
the perspective on the photograph does not make it very clear, but the
right leg is the "short" one
different angular opening from one foot to the other; higher left
shoulder with respect to the right
permanently extended torso muscles (unconscious reflex to hinder
movement of the first 3 or 4 ribs)
If your child is asthmatic, place him/her in the same positions, ask him/her
to lie down "right" and look for the above points. In some (rare) cases
the above description is reversed, and sometimes other descriptions (very
rare) are not in this system of rotation, but are characterised by two
shoulders being "blocked" forward.
Description of the mechanisms involved
How can these articular "messages" be wrongly interpreted ?
 Merely because when they reach the nervous ganglia level (in which
visceral or cutaneous information is also present) a confusion occcurs,
precisely as in the case of heart attacks where the painful message
coming from the heart is regarded as coming from the left arm. The
latter is referred to a a ghost information.
Merely because when they reach the nervous ganglia level (in which
visceral or cutaneous information is also present) a confusion occcurs,
precisely as in the case of heart attacks where the painful message
coming from the heart is regarded as coming from the left arm. The
latter is referred to a a ghost information.
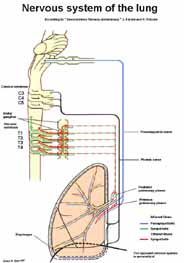
In the body, all functions are governed by two major systems: the
sympatic and the parasympatic. On the whole, to simplify, the
parasympatic has a constricting role and the sympatic has an
accelerating role.
It is the case for bronchuses: sympatic fibers of medullary origin,
originating from upper thoracic levels (T1, T2, T3 and T4) are "broncho-dilatating,"
whereas parasympatic fibers originate from the pneumogastric nerve (C3,
C4 and C5) and are "broncho-constrictives."
If this balance is broken due to deficient actions from the sympatic
fibers, a bronchial fricative reaction occurs. With every inspiration, a
bit deep, resulting from a physical effort, etc., by laughter, by
coughing, the rising upper ribs movement is going to be disrupted by
their bad position, the inspired volume is going to be reduced, and some
anomalous articular messages are going to be produced.
Note: because these messages are unconsciously the origin of the crisis, the asthmatic blocks the rib cage in a position of closing and adopts abdominal breathing that doesn't solicit its superior coasts. Its shoulders went up again and «forward» by the contraction of its pectoral muscles that is always aimed to the extreme, even to rest. Everybody can verify it, it is sufficient to feel the entrance of the armpit to have proof of it.
The technique of treatment
It is very simple and is accessible to all physicians or
physiotherapists already knowing how to exercise techniques of
structural ostéo-articular manipulation (osteopathy, chiropractie,
etc.). A simple specific formation of three day, to their cabinet and
on the quoted pathologies, is sufficient to immediately become
operational. My technique is very gentle, since it permits me to treat
a child of three weeks as well as one 75 years and more.
The treatment includes to:
- give back a normal mobility to a certain number of unsettled joints, feet, legs, basin, lumbar, dorsal and cervical rachis (by the personal, very gentle techniques, based on the stake in stance and on the breathing)
- perfectly restructure the rib cage while suppressing all rib subluxations (by the personal techniques, that are not taught in any school, and adapted according to the age of the subject)
- allow the subject, while being standing, to perfectly be in his/her/its axes while having recourse, so necessary, to a specific podiatry work (that doesn't have anything to see with the exercised methods, of which some is simply a matter for the swindle)
- educate the subject in posturology so that he/it learns to remain in his/her/its axes in the standing position, foundation either lying; to give it back responsibility and to prevent him/her from remaining in his/her unconscious habits (for example, for children, to sprawl on a sofa to look for hours at the television!).
Three to four sittings of a working hour will be necessary to get a lasting stabilization.
The rate of success
It passes 90% and the only failures (although there
is a specific improvement of life comfort) are owed to problems of age
and the bony illnesses forbidding the articular mobilizations.
Surinfectious from antibio-resistant bacteria or from mushrooms
(Candidas Albicans, very frequent), require a tracking (exam of spit)
that will bring the solution by orientation toward one or several
antibiotics partners, or a antifongic treatment.
It is the work of the usual physician.
I have used my method since 1985 with a rate of success that made the
thread of the experience and other practitioners only increase also
with the same results. I then discuss recovery because I have more
than 5 years without noted relapses (norm admitted in the medical
middle).
Since the first sitting, the patient recovers the totality of his/her
vital capacity (inspired air volume) with a gain for an adult of 3/4
of liter to 1 liter of air (true to the spirometre). It can again «to
breathe to full lungs» and, made no crisis very often when one sees it
later for the second sitting one week again. I do not lie or cheat on
this topic, my results offer proof of the accurateness of the
reasoning and the reality of the therapeutic act.
Besides, this type of care is to the exclusive load of the patient and
cannot give place to any repayment: it must therefore be efficient!
To make quit a crisis of asthma
Nothing simpler, the necessary material in case of crisis holds in the
hand of the sick that is... his/her index finger!
In the nearly totality of cases, ribs subluxations (close the
window to come back here) are on the right "postériorisées" and the
trigger points the crisis is situated on the previous joint of the
second or third ribs.
The point of stopping the crisis is always of the opposite side.
It is situated under the left armpit, between coasts (2 and 3 or 3 and
4) and is very painful to the touch. It is not difficult, when one
finds it with the index finger and pushes, it provokes a reflex of
grimace and loop line. Under the finger, one feels «like a mobile
grease ball», it is there that it is necessary to do a slow massage, (with
limited pressure, to be tolerable) in the sense of coasts while
remaining good in the intercostal space.
At the same time as this massage, it is necessary to do deep
inspirations and at the end of 4 or 5, the crisis stops
instantaneously. This point even acts outside of all crisis: it
immediately increases the vital capacity. All asthmatics (not
inspiratory dyspnea) can verify immediately the presence and the
efficiency of this point that all media has refusedto publish in the
last 10 years.
To the "Marjolaine" lounge, in 1996, I did a conference on the asthma
and at the end of the exposition, everybody wanted explanations on
this point.
I therefore brought up 3 asthmatic people on the stage and triggered
them to a crisis. Then I demonstrated that it was simple to make it
stop. As the microphone was placed close to each person's mouth, all
in the room heard clearly the respiratory noises related to the crisis,
noted expiratory difficulty and heard the return to a normal situation
in a few big inspirations with the use of the method. The whole room
applauded, and this demonstration provided the proof of the accuracy
of my works.
The conference having been recorded, all cassettes have been bought to
the point that I should have waited that one duplicates me one of it
for my personal use. They circulated (and circulate again!) and many
practitioners, whose patients spoke about me, contacted me to learn
more about my research.
Today, everybody can learn about my works on my Internet site, study
already published articles, learn about my two books. They can
discover another reason for the upsurge in cases of asthma of the
child, know all steps that I took (without success!) since 1985 to
inform politicians, medical professionals, the media, and they can
discover the practitioners who use my method.
No longer can groups of people in authority block information as was
done in the last ten years.